Consider sildenafil for patients with right heart failure (RHF) and pulmonary hypertension, but only after careful evaluation of potential benefits and risks. This isn’t a first-line treatment, but it may offer a valuable therapeutic option in specific circumstances.
Studies suggest sildenafil’s phosphodiesterase-5 (PDE5) inhibitory action can improve pulmonary vascular resistance and reduce right ventricular afterload. This translates to potential improvements in exercise capacity and quality of life for select patients. However, individual responses vary greatly.
Before prescribing sildenafil, thoroughly assess the patient’s hemodynamic profile and overall health. Monitor blood pressure and liver function closely. Remember that hypotension is a common side effect, demanding cautious administration, particularly in patients with pre-existing cardiovascular conditions. Regular monitoring is paramount.
Specific patient populations, such as those with severe hepatic impairment or significant hypotension, should be approached with additional caution, or sildenafil might be contraindicated entirely. The patient’s complete medical history is critical in determining suitability. Close collaboration with a cardiologist is highly recommended.
Always refer to updated clinical guidelines and the most recent research before making treatment decisions. Individualized treatment plans, based on rigorous assessment and ongoing monitoring, are vital for maximizing efficacy and minimizing adverse events in RHF management.
- Sildenafil in Right Heart Failure: A Focused Overview
- Mechanisms of Action in RHF
- Clinical Considerations and Recommendations
- Ongoing Research and Future Directions
- Mechanism of Sildenafil Action in Pulmonary Hypertension
- Clinical Trials and Efficacy Data for Sildenafil in Right Heart Failure
- Specific Trial Results and Considerations
- Adverse Effects and Contraindications of Sildenafil in Right Heart Failure Patients
- Headache and Flushing
- Visual Disturbances
- Contraindications
- Monitoring and Management
- Current Clinical Guidelines and Future Directions for Sildenafil in Right Heart Failure
- Pulmonary Hypertension and Sildenafil
- Future Research Directions
- Summary of Current Evidence and Unanswered Questions
- Patient Selection and Monitoring
Sildenafil in Right Heart Failure: A Focused Overview
Sildenafil, primarily known for its use in erectile dysfunction, shows promise in treating right heart failure (RHF) by improving pulmonary vascular resistance. Clinical trials suggest a potential benefit, particularly in patients with pulmonary hypertension associated with RHF. However, its efficacy varies depending on the underlying cause and severity of RHF.
Mechanisms of Action in RHF
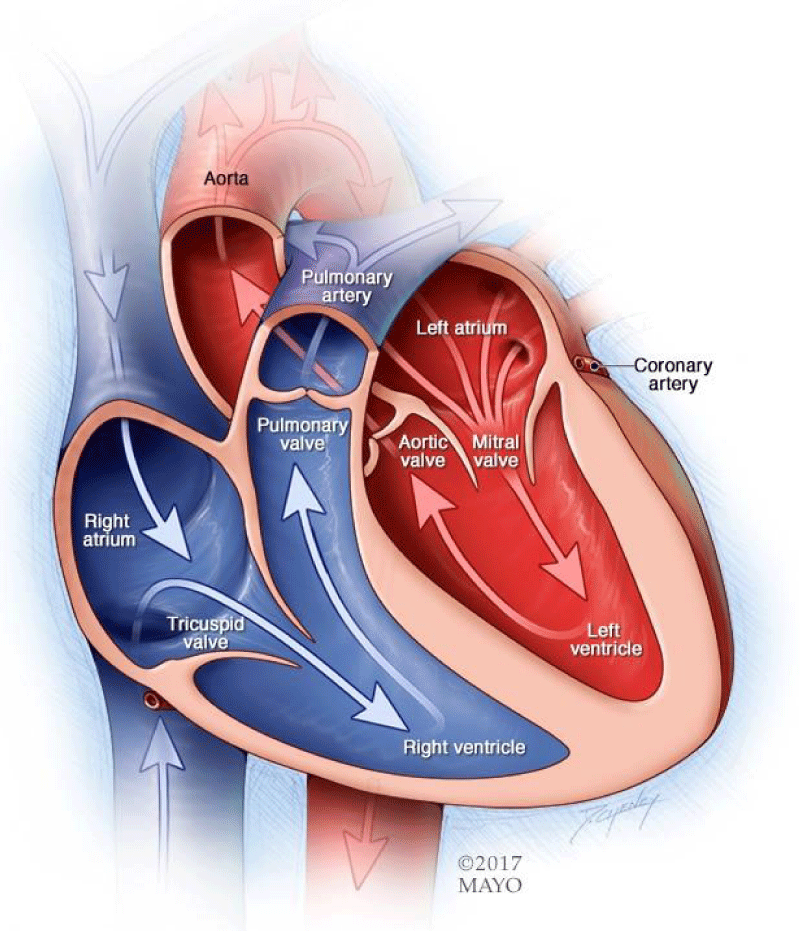
Sildenafil inhibits phosphodiesterase-5 (PDE5), increasing levels of cyclic guanosine monophosphate (cGMP). This leads to smooth muscle relaxation in pulmonary arteries, reducing pulmonary vascular resistance and improving right ventricular function. This mechanism can alleviate symptoms and potentially improve survival in specific patient populations.
Clinical Considerations and Recommendations
Current guidelines don’t routinely recommend sildenafil for all RHF patients. It’s generally considered for those with pulmonary hypertension secondary to RHF who haven’t responded adequately to other therapies. Careful monitoring of blood pressure, particularly the systemic blood pressure and potential for hypotension is vital. Patients with severe hepatic or renal impairment should be carefully evaluated before sildenafil prescription due to potential increased risk of side effects. Individual patient response varies, necessitating careful assessment and ongoing monitoring.
Ongoing Research and Future Directions
Further research is needed to fully define the role of sildenafil in RHF. Studies focusing on specific RHF subtypes and patient selection criteria are crucial for establishing clearer treatment guidelines. Investigating optimal dosing strategies and combining sildenafil with other treatments also requires further investigation. Larger, well-designed trials are critical for definitively determining the benefits and risks of sildenafil in this population.
Mechanism of Sildenafil Action in Pulmonary Hypertension
Sildenafil treats pulmonary hypertension by specifically targeting the pulmonary vasculature.
Primarily, it inhibits phosphodiesterase-5 (PDE5). This enzyme usually breaks down cyclic guanosine monophosphate (cGMP), a crucial molecule for smooth muscle relaxation.
- By blocking PDE5, sildenafil elevates cGMP levels.
- Increased cGMP activates protein kinase G (PKG).
- PKG triggers a cascade, leading to decreased calcium influx into pulmonary artery smooth muscle cells.
- Reduced intracellular calcium causes smooth muscle relaxation and subsequent vasodilation.
This vasodilation reduces pulmonary vascular resistance, improving blood flow to the lungs and lowering pulmonary arterial pressure. Consequently, the right ventricle’s workload decreases, potentially improving its function.
Furthermore, sildenafil exhibits other beneficial effects:
- It can improve endothelial function by increasing nitric oxide (NO) bioavailability.
- It may possess anti-inflammatory properties, though further research is needed in this area.
- Studies suggest possible effects on pulmonary vascular remodeling, although the precise mechanisms require clarification.
The precise contribution of each of these mechanisms to the overall therapeutic effect remains an active area of investigation. However, the primary mechanism hinges on its specific PDE5 inhibitory action, leading to pulmonary vasodilation and reduced right ventricular afterload.
Clinical Trials and Efficacy Data for Sildenafil in Right Heart Failure
While sildenafil’s primary use targets pulmonary arterial hypertension (PAH), its effects on right heart failure (RHF) warrant investigation. Several studies explored sildenafil’s impact on RHF symptoms and hemodynamics, though results are mixed. The REVEAL trial, for instance, showed a statistically significant improvement in 6-minute walk distance in patients with PAH-associated RHF treated with sildenafil compared to placebo. This suggests potential benefit in improving exercise capacity. However, other studies haven’t consistently replicated these findings, highlighting the need for further research to determine sildenafil’s precise role in RHF management. More robust, larger-scale clinical trials are necessary to establish clear efficacy and safety profiles in various RHF subtypes.
Specific Trial Results and Considerations
Data from specific trials must be interpreted cautiously, considering factors like patient heterogeneity, varying disease severities, and concomitant medications. For example, some studies found improvements in biomarkers like N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels in certain RHF patient groups following sildenafil treatment, suggesting potential positive effects on cardiac remodeling. Conversely, some trials reported no significant benefit on mortality or hospitalization rates. This highlights the need for careful patient selection and a thorough evaluation of individual risk-benefit profiles before initiating sildenafil therapy for RHF. Current evidence doesn’t support widespread sildenafil use for RHF, but ongoing research may change this. Clinicians should consult current guidelines and stay updated on emerging research to make informed decisions.
Adverse Effects and Contraindications of Sildenafil in Right Heart Failure Patients
Sildenafil, while potentially beneficial for some aspects of right heart failure, carries risks. Hypotension is a significant concern, particularly in patients already experiencing low blood pressure. This risk is amplified by concurrent use of nitrates or other vasodilators. Monitor blood pressure closely, especially after initiating sildenafil therapy.
Headache and Flushing
Headache and facial flushing are common side effects. These typically resolve spontaneously but warrant attention if severe or persistent. Patients should be advised of these potential effects and instructed to report any significant discomfort.
Visual Disturbances
Visual disturbances, such as blurred vision or changes in color perception, are also reported. These effects usually subside upon discontinuation of the drug, but careful ophthalmological assessment is recommended, particularly in patients with pre-existing eye conditions.
Contraindications
Sildenafil is contraindicated in patients with severe hepatic or renal impairment, due to altered drug metabolism and excretion. It’s also contraindicated in patients with a history of myocardial infarction or unstable angina, as it might increase myocardial oxygen demand. Concurrent use of strong CYP3A4 inhibitors (such as ketoconazole or ritonavir) should be avoided due to the risk of increased sildenafil plasma concentration and intensified side effects. Patients with severe pulmonary hypertension should be carefully evaluated due to the potential risk of worsening symptoms, and the benefits weighed carefully against the risks.
Monitoring and Management
Regular monitoring of blood pressure, heart rate, and oxygen saturation is crucial during sildenafil treatment. Patients should be educated on the potential side effects and advised to report any concerning symptoms immediately. Close collaboration between cardiologists and prescribing physicians is essential for optimal management.
Current Clinical Guidelines and Future Directions for Sildenafil in Right Heart Failure
Currently, no major clinical guidelines explicitly recommend sildenafil for right heart failure (RHF) as a first-line therapy. However, its potential benefit in specific RHF subtypes, particularly those associated with pulmonary hypertension, is being actively explored.
Pulmonary Hypertension and Sildenafil
Sildenafil’s vasodilatory effects on the pulmonary vasculature make it a potential therapeutic option for RHF patients with elevated pulmonary vascular resistance. Studies focusing on this population show promise, but larger, well-designed clinical trials are needed to establish clear treatment guidelines. The current research focuses on identifying subgroups most likely to benefit and determining optimal dosing strategies.
Future Research Directions
Future research should prioritize identifying predictive biomarkers for sildenafil responsiveness in RHF. This will help tailor treatment and minimize adverse events. Researchers are also investigating sildenafil’s potential synergistic effects when combined with other established RHF therapies. Exploration of novel delivery methods and formulations could enhance efficacy and reduce side effects. Furthermore, a thorough investigation into long-term effects and cost-effectiveness is required.
Summary of Current Evidence and Unanswered Questions
| Aspect | Current Status | Future Directions |
|---|---|---|
| Clinical Guideline Recommendations | No explicit recommendations for RHF | Develop evidence-based guidelines based on robust clinical trials |
| Patient Selection | Focus on patients with pulmonary hypertension | Identify predictive biomarkers for treatment response |
| Combination Therapies | Limited data on synergistic effects with other therapies | Investigate combination therapies and optimize treatment regimens |
| Long-Term Outcomes | Data scarce | Assess long-term efficacy, safety, and cost-effectiveness |
Patient Selection and Monitoring
Careful patient selection is crucial. Regular monitoring of blood pressure, pulmonary artery pressure, and other relevant parameters is necessary to assess treatment response and manage potential adverse effects. Clinicians must carefully weigh the potential benefits against potential risks, especially in patients with certain comorbidities.